Publication¶
Registry Forge: an open-source end-to-end pipeline for patient-directed SMART on FHIR registries¶
Danielle Boyce, MPH, DPA1,2; Alan Premasiri1; Shawn Sullivan1; Beth Levine1; Fernando G. Vieira, MD1
1 ALS Therapy Development Institute, 480 Arsenal Street, Suite 201, Watertown, MA 02472, USA 2 Johns Hopkins University, Biomedical Informatics and Data Science Section, Baltimore, MD 21205, USA
Corresponding author: Danielle Boyce, dboyce@als.net
Preprint, not peer reviewed
This is a preprint. It is a preliminary report that has not been certified by peer review. It should not be relied on to guide clinical practice or health-related behavior and should not be reported in news media as established information. A version of this manuscript has been submitted to JAMIA Open.
Cite this preprint
Boyce D, Premasiri A, Sullivan S, Levine B, Vieira FG. Registry Forge: an open-source end-to-end pipeline for patient-directed SMART on FHIR registries. Preprint. 2026. doi:[DOI PENDING — to be minted via DataCite]
Download the full preprint (PDF) Source repository
| Article type | Application Note |
| Preprint DOI | Pending (DataCite) |
| Software / release archive DOI | 10.71944/2P5C-NG50 |
| Submitted to | JAMIA Open |
| License | MIT (software); CC BY (preprint text), unless noted otherwise |
| Keywords | Patient Registries; SMART on FHIR; HL7; Electronic Health Records; Amyotrophic Lateral Sclerosis |
Abstract¶
Objectives. Patient-directed SMART on FHIR lets registries acquire longitudinal electronic health record data, but the payload requires substantial engineering before use. We present Registry Forge, an open-source pipeline that converts it into research-ready outputs.
Materials and Methods. Registry Forge decodes and parses mixed C-CDA, HTML, RTF, PDF, and FHIR inputs, joins records to a canonical patient identifier, and emits a browser-viewable dashboard, an OMOP CDM v5.4 data set, GA4GH Phenopackets v2, a code inventory, and regex extractions of disease-specific narrative content.
Results. Applied to the ALS Research Collaborative Study (94 participants, 56 US health systems), it processed 22,686 source files and 1,791 FHIR Bundles (109,599 resources); only 15.0% of files were full C-CDA.
Discussion. This pipeline generalizes to any registry acquiring data through patient-directed SMART on FHIR.
Conclusion. Registry Forge closes the acquisition-to-analysis gap with no server infrastructure and is openly available.
Lay summary¶
Patient registries and natural history studies (referred to as 'registries' in this article) are research databases that collect data on people with a particular medical condition, often over time. To work well, they need detailed medical records, either from the participant answering surveys or through information from each participant's doctors. A federal rule lets participants log in to their hospital's patient portal and grant a registry access to their own electronic health record. This solves the data collection problem but creates a new one: the downloaded files arrive in many formats and have to be cleaned, combined, and standardized before researchers can use them. Small registries, especially those for rare diseases, often cannot afford the engineers required to do this work.
We built Registry Forge, a free open-source software tool that does this work automatically. We used it for the ALS Research Collaborative Study, a long-running natural history study of amyotrophic lateral sclerosis run by the ALS Therapy Development Institute. Registry Forge processed records from 94 study participants whose care spanned more than 50 US health systems and turned them into research-ready data sets. The tool runs on a standard laptop and is free for anyone to use.
Figures¶
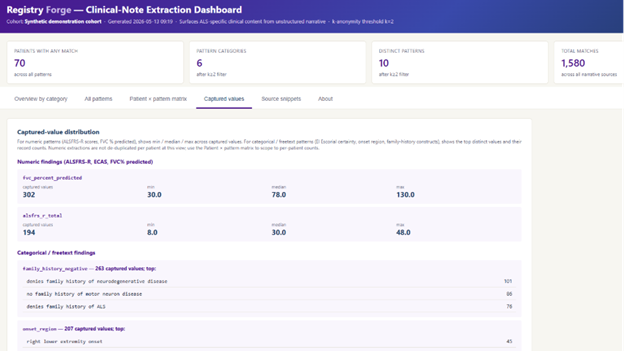
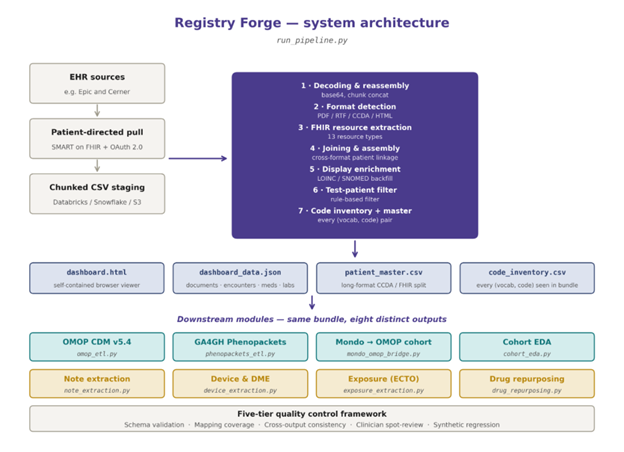
run_pipeline.py) ingests SMART on FHIR-acquired C-CDA, RTF, PDF, HTML, and FHIR inputs, joins them to a canonical patient identifier, and emits a single JSON bundle. The bundle feeds a static HTML dashboard and eight independent add-on modules (OMOP CDM v5.4, GA4GH Phenopackets, Mondo to OMOP bridge, cohort EDA, note extraction, device and DME, environmental exposure, and drug repurposing), all under a five-tier quality-control framework.Try it¶
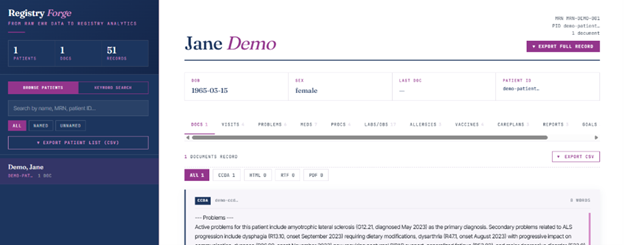
A fully synthetic, single-patient interactive demonstration of the dashboard is hosted alongside the source code so that other registries can evaluate the pipeline before adopting it. See the live demos and the architecture pages.
Funding¶
This work was supported in part by the Centers for Disease Control and Prevention (Grant No. R01-TS000341), the ALS Therapy Development Institute, the Brothers Brook Foundation, and The William K. Bowes, Jr. Foundation. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Competing interests¶
The authors are employees of the ALS Therapy Development Institute, the non-profit research organization that operates the ALS Research Collaborative Study and supported this work. The authors declare no other competing interests.
Data and code availability¶
Source code for the complete pipeline, the browser dashboard, and a fully synthetic single-patient demonstration cohort are publicly available at https://alstdi.github.io/RegistryForgeALS/ (repository: https://github.com/alstdi/RegistryForgeALS) under the MIT License. The exact release used for this manuscript is archived with a citable DOI (10.71944/2P5C-NG50) through ALS TDI's DataCite membership. The clinical data described cannot be openly shared due to the terms of the ALS Research Collaborative Study informed consent. A de-identified version is available to qualified researchers through the ARC Data Commons.